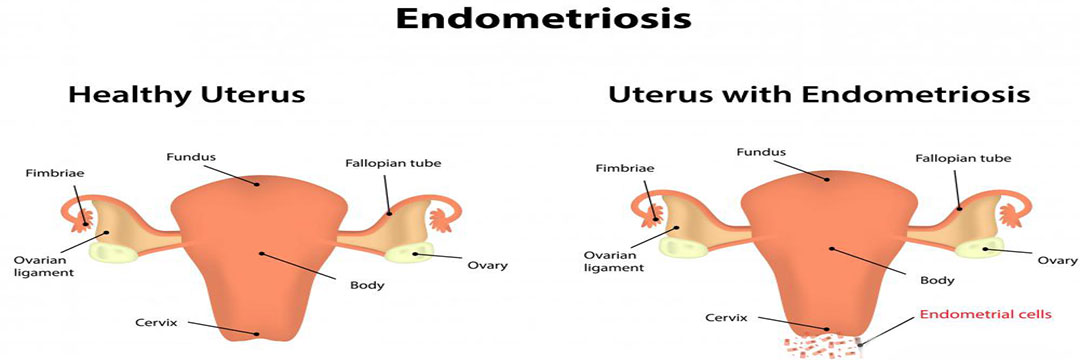
What is endometriosis?
Endometriosis is the abnormal growth of endometrial tissue similar to that which lines the interior of the uterus, but in a location outside of the uterus. Endometrial tissue is shed each month during menstruation. Areas of endometrial tissue found in ectopic locations are called endometrial implants. These lesions are most commonly found on the ovaries, the Fallopian tubes, the surface of the uterus, the bowel, and on the membrane lining of the pelvic cavity (i.e. the peritoneum). They are less commonly found to involve the vagina, cervix, and bladder. Rarely, endometriosis can occur outside the pelvis. Endometriosis has been reported in the liver, brain, lung, and old surgical scars. Endometrial implants, while they may become problematic, are usually benign (i.e. non-cancerous).
What are the stages of endometriosis?
Endometriosis is classified into one of four stages (I-minimal, II-mild, III-moderate, and IV-severe) based upon the exact location, extent, and depth of the endometriosis implants as well as the presence and severity of scar tissue and the presence and size of endometrial implants in the ovaries. Most cases of endometriosis are classified as minimal or mild, which means there are superficial implants and mild scarring. Moderate and severe endometriosis typically result in cysts and more severe scarring. The stage of endometriosis is not related to the degree of symptoms a woman experiences, but infertility is common with stage IV endometriosis.
What are the signs and symptoms endometriosis?
Most women who have endometriosis, in fact, do not have symptoms. Of those who do, the most common include:
- Pain (usually pelvic) that usually occurs just before menstruation and lessens after menstruation
- Painful sexual intercourse
- Cramping during intercourse
- Cramping or pain during bowel movements or urination
- Infertility
- Pain with pelvic examinations
The intensity of the pain can vary from month to month, and can vary greatly among affected individuals. Some women experience progressive worsening of symptoms, while others can have resolution of pain without treatment.
Pelvic pain in women with endometriosis depends partly on where endometrial implants of endometriosis are located.
- Deeper implants and implants in areas of high nerve density are more apt to produce pain.
- The implants may also release substances into the bloodstream which are capable of eliciting pain.
- Pain can result when endometriotic implants incite scarring of surrounding tissues. There appears to be no relationship between severity of pain and the amount of anatomical disease which is present.
Endometriosis can be one of the reasons for infertility for otherwise healthy couples. When laparoscopic examinations are performed during evaluations for infertility, implants are often found in individuals who are totally asymptomatic. The reasons diminished fertility in many patients with endometriosis are not understood. Endometriosis may incite scar tissue formation within the pelvis. If the ovaries and Fallopian tubes are involved, the mechanical processes involved in the transfer of fertilized eggs into the tubes may be altered. Alternatively, the endometriotic lesions may produce inflammatory substances which adversely affect ovulation, fertilization, and implantation.
Other symptoms that can be related to endometriosis include
- lower abdominal pain,
- diarrhea and/or constipation,
- low back pain,
- chronic fatigue
- irregular or heavy menstruation,
- painful urination, or
- bloody urine (particularly during menstruation).
Rare symptoms of endometriosis include chest pain or coughing blood due to endometriosis in the lungs and headache and/or seizures due to endometriosis in the brain.
Does endometriosis increase a woman’s risk of getting cancer?
Some studies have postulated that women with endometriosis have an increased risk for development of certain types of ovarian cancer, known as epithelial ovarian cancer (EOC). This risk is highest in women with both endometriosis and primary infertility (those who have never conceived a pregnancy). The use of combination oral contraceptive pills (OCPs), which are sometimes used in the treatment of endometriosis, appears to significantly reduce this risk.
The reasons for the association between endometriosis and ovarian epithelial cancer are not clearly understood. One theory is that the endometriosis implants themselves undergo malignanttransformation to cancer. Another possibility is that the presence of endometriosis may be related to other genetic or environmental factors that serve to increase a women’s risk of developing ovarian cancer.
What causes endometriosis?
The cause of endometriosis is unknown. One theory is that the endometrial tissue is deposited in unusual locations by the retrograde flow of menstrual debris through the Fallopian tubes into the pelvic and abdominal cavities. The cause of this retrograde menstruation is not clearly understood. It is clear that retrograde menstruation is not the only cause of endometriosis, as many women who have retrograde menstruation do not develop the condition.
Another possibility is that areas lining the pelvic organs possess primitive cells that are able to develop into other forms of tissue, such as endometrium. (This process is termed coelomic metaplasia.)
It is also likely the direct transfer of endometrial tissues at the time of surgery may be responsible for the endometriosis implants occasionally found in surgical scars (for example, episiotomy or Cesarean section scars). Transfer of endometrial cells via the bloodstream or lymphatic system is the most plausible explanation for the rare cases of endometriosis that are found in the brain and other organs remote from the pelvis.
Finally, there is evidence that some women with endometriosis have an altered immune response in women with endometriosis, which may affect the body’s natural ability to recognize ectopic endometrial tissue.
What medications treat endometriosis?
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Nonsteroidal anti-inflammatory drugs or NSAIDs (such as ibuprofen or naproxen sodium) are commonly prescribed to help relieve pelvic pain and menstrual cramping. These pain-relieving medications have no effect on the endometrial implants or the progression of endometriosis. However, they do decrease prostaglandin production, and prostaglandins are well-known to have a role in the causation of pain. As the diagnosis of endometriosis can only be definitively confirmed with a biopsy, many women with complaints suspected to arise from endometriosis are treated for pain first without a firm diagnosis being established. Under such circumstances, NSAIDs are commonly used as a first line empirical treatment. If they are effective in controlling the pain, no other procedures or medical treatments are needed. If they are ineffective, additional evaluation and treatment will be necessary.
Since endometriosis occurs during the reproductive years, many of the available medical treatments for endometriosis rely on interruption of the normal cyclical hormone production by the ovaries. These medications include GnRH analogs, oral contraceptive pills, and progestins.
Gonadotropin-releasing hormone analogs (GnRH analogs)
Gonadotropin-releasing hormone analogs (GnRH analogs) have been effectively used to relieve pain and reduce the size of endometriosis implants. These drugs suppress estrogen production by the ovaries by inhibiting the secretion of regulatory hormones from the pituitary gland. As a result, menstrual periods stop, mimicking menopause. Nasal and injection forms of GnRH agonists are available.
The side effects are a result of the lack of estrogen, and include:
- hot flashes,
- vaginal dryness,
- irregular vaginal bleeding,
- mood alterations,
- fatigue, and
- loss of bone density (osteoporosis).
Fortunately, by adding back small amounts of progesterone in pill form (similar to treatments sometimes used for symptom relief in menopause), many of the annoying side effects due to estrogen deficiency can be avoided. “Add back therapy” is a term that refers to this modern way of administering GnRH agonists along with progesterone in a way to ensure compliance by eliminating most of the unwanted side effects of GnRH therapy.
Oral contraceptive pills
Oral contraceptive pills (estrogen and progesterone in combination) are also sometimes used to treat endometriosis. The most common combination used is in the form of the oral contraceptive pill (OCP). Sometimes women who have severe menstrual pain are asked to take the OCP continuously, meaning skipping the placebo (hormonally inert) portion of the cycle. Continuous use in this manner will generally stop menstruation altogether. Occasionally, weight gain, breast tenderness, nausea, and irregular bleeding may occur. Oral contraceptive pills are usually well-tolerated in women with endometriosis.
Progestins
Progestins [for example, medroxyprogesterone acetate (Provera, Cycrin, Amen), norethindrone acetate, norgestrel acetate (Ovrette)] are more potent than birth control pills and are recommended for women who do not obtain pain relief from or cannot take a birth control pill. They may be helpful in women who do not respond, or cannot take (for medical reasons) oral contraceptives.
Side effects are more common and include:
- breast tenderness,
- bloating,
- weight gain,
- irregular uterine bleeding, and
- depression.
Because the absence of menstruation (amenorrhea) induced by high doses of progestins can last many months following cessation of therapy, these drugs are not recommended for women planning pregnancy immediately following cessation of therapy.
Other drugs used to treat endometriosis
Danazol (Danocrine)
Danazol (Danocrine) is a synthetic drug that creates a high androgen (male type hormone) and low estrogen hormonal environment by interfering with ovulation and ovarian production of estrogen. Eighty percent of women who take this drug will have pain relief and shrinkage of endometriosis implants, but up to 75% of women develop significant side effects from the drug. These include:
- weight gain,
- edema (swelling),
- breast shrinkage,
- acne,
- oily skin,
- hirsutism (male pattern hair growth),
- deepening of the voice,
- headache,
- hot flashes,
- changes in libido, and
- mood alterations.
Except for the voice changes, all of these side effects are reversible. In some cases, resolution of the side effects may take many months. Danazol should not be taken by women with certain types of liver, kidney, or heart conditions. This product is rarely used.
Aromatase inhibitors
A more current approach to the treatment of endometriosis has involved the administration of drugs known as aromatase inhibitors (for example, anastrozole [Arimidex] and letrozole [Femara]). These drugs act by interrupting local estrogen formation within the endometriosis implants themselves. They also inhibit estrogen production within the ovary and adipose tissue. Research is ongoing to evaluate the effectiveness of aromatase inhibitors in the management of endometriosis. Aromatase inhibitors can cause significant bone loss with prolonged usage. They must also be employed in combination with other drugs in premenopausal women because of their effects on the ovaries.
Can surgery cure endometriosis?
Surgical treatment for endometriosis can be useful when the symptoms are severe or there has been an inadequate response to medical therapy. Surgery is the preferred treatment when there is anatomic distortion of the pelvic organs or obstruction of the bowel or urinary tract. It may be classified either as conservative, in which the uterus and ovarian tissue are preserved, or definitive, which involves hysterectomy (removal of the uterus), with or without removal of the ovaries.
Conservative surgery is typically performed laparoscopically. Endometrial implants may be excised or destroyed by different sources of energy (e.g. laser, electrical current). If the disease is extensive and anatomy is distorted, laparotomy may be required.
While surgical treatments can be very effective in the reduction of pain, the recurrence rate of endometriosis following conservative surgical treatment has been estimated to be as high as 40%. Many doctors recommend ongoing medical therapy following surgery in an attempt to prevent symptomatic disease recurrence.
Who gets endometriosis?
Endometriosis affects women during their reproductive years. The exact prevalence of endometriosis is not known, since many women who are later identified as having the condition are asymptomatic. Endometriosis is estimated to affect over one million women (estimates range from 3% to 18% of women) in the United States. It is one of the leading causes of pelvic pain and it is responsible for many of the laparoscopic procedures and hysterectomies performed by gynecologists. Estimates suggest that 20% to 50% of women being treated for infertility have endometriosis, and up to 80% of women with chronic pelvic pain may be affected.
While most cases of endometriosis are diagnosed in women aged 25 to 35 years, endometriosis has been reported in girls as young as 11 years of age. Endometriosis is rare in postmenopausal women. Studies further suggest that endometriosis is most common in taller, thin women with a low body mass index (BMI). Delaying pregnancy until an older age, never giving birth, early onset of menses, and late menopause all have been shown to be risk factors for endometriosis. It also is likely that there are genetic factors which predispose a woman to developing endometriosis, since having a first-degree relative with the condition increases the chance that a woman will develop the condition.
Post a comment