What is the appendix?
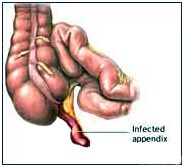
If the appendix becomes infected (appendicitis), the infected appendix must be surgically removed (emergency appendectomy) before a hole develops in the appendix (perforation) and spreads the infection to the entire abdominal space (peritonitis).
The appendix is a narrow, small, finger-shaped portion of the large intestine that generally hangs down from the lower right side of the abdomen.
 What is appendicitis and what causes it?
What is appendicitis and what causes it?
Appendicitis is a sudden inflammation of the appendix. Although the appendix does not seem to serve any purpose, it can become diseased and, if untreated, can burst, causing infection and even death.
The cause of appendicitis is usually unknown. Appendicitis may occur after a viral infection in the digestive tract or when the tube connecting the large intestine and appendix is blocked or trapped by stool. It is thought that blockage of the opening of the appendix into the bowel by a hard, small stool fragment causes inflammation and infection of the appendix (appendicitis). The inflammation can cause infection, a blood clot, or rupture of the appendix.
The infected appendix then must be surgically removed (emergency appendectomy) before a hole develops in the appendix and spreads the infection to the entire abdominal space.
What are the symptoms of appendicitis?
- Abdominal pain – pain may begin in the upper-middle abdomen then develop to sharp localized pain
- Abdominal pain may be worse when walking or coughing
- Fever usually occurs within several hours
- Loss of appetite
- Nausea
- Vomiting
- Constipation
- Rectal tenderness
- Chills and shaking
If you have these symptoms, see a doctor immediately! Because of the risk of rupture, which may happen as soon as 48 to 72 hours after symptoms begin, appendicitis is considered an emergency.
How is appendicitis treated?
The best treatment of appendicitis is its surgical removal. Mild appendicitis may sometimes be cured with antibiotics. More serious cases are treated with surgery to remove the appendix, called an appendectomy. Doctors either use an “open” technique or a minimally invasive approach to remove the appendix.
Appendicitis is considered an emergency and anyone with symptoms needs to see a doctor immediately!
What is a laparoscopic appendectomy?
The laparoscopic (minimally invasive) surgical technique involves making several tiny cuts in the abdomen and inserting a miniature camera and surgical instruments. As many as three or four incisions are made. The surgeon then removes the appendix with the instruments, so there is usually no need to make a large incision in the abdomen. The camera projects a magnified image of the area onto a television monitor which helps guide the surgeons as they remove the appendix.
What is the benefit of laparoscopic appendectomy?
Most cases of acute appendicitis can be treated laparoscopically. The main advantages are : -
- Less post-operative pain
- Faster recovery and return to normal activity
- Shorter hospital stay
- Less post-operative complications
- Minimally sized incisions/scars
In most cases, patients can be discharged within 24 to 36 hours. By contrast, the hospital stay is typically two to five days for an open procedure.
Can every patient have a laparoscopic appendectomy?
No. Patients with cardiac diseases and COPD would not be good candidates for laparoscopic appendectomy. In addition, laparoscopic appendectomy is not recommended for those with pre-existing disease conditions.
Laparoscopic appendectomy may also be more difficult in patients who have had previous lower abdominal surgery and for obese patients. The elderly may also be at increased risk for complications with general anesthesia. We evaluate every patient to determine the appropriate type of surgery to perform.
Treatment Options:
The appendix is then removed using a camera through the belly button as well as two other small incisions. Depending on how advanced the infection is, the patient is kept on antibiotics. If the infection is very advanced, the operation may be delayed while the patient receives antibiotics for several weeks. After the infection has improved, a laparoscopic appendectomy is performed.
Laparoscopic appendectomy is a safe and effective treatment for appendicitis. However, in the presence of infection, adhesions, or variations in anatomy, this method becomes dangerous and your surgeon may need to make the prudent decision to continue by making the traditional incision to safely complete the operation. This should not be seen as a failure, but as a wise decision by your surgeon to prevent dangerous complications. Other complications, although rare, include bleeding and infection. It is extremely uncommon to require a blood transfusion for this operation.
This operation is generally performed with general anesthesia. An IV line will be placed in your arm for fluids and you will be brought into the operation room. The anesthesiologist and nurses will use monitors to check your heart rate and breathing during the procedure. These may include EKG leads, a blood pressure cuff, an oxygen mask and sleeves on your legs to prevent clots from forming.
Once you are asleep, the operating room team will work together to perform your operation. When your operation is complete, you will be awakened from anesthesia in the operating room but you may not remember this. After a few hours in the recovery room, the nurses will help you out of bed and give you something to drink. It is common to feel groggy and nauseated soon after surgery and medication is available to help with these discomforts. This information is not intended to replace a visit with your physician.
Picturised Procedure of Laparoscopic Appendectomy:
Laparoscopic Appendectomy
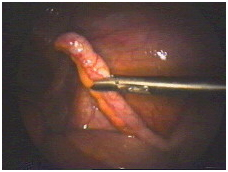
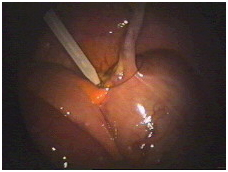
This is a normal appendix in a female patient found to have an infection of the reproductive organs. Since the appendix serves no useful function, it will be removed to save her from ever getting appendicitis in the future
The first step is to free up the appendix down to where it is attached to the large bowel. This requires dividing the mesentery which contains the blood vessels that supply the appendix. Bipolar forceps apply an electric current which seals the blood vessels and prevents bleeding.
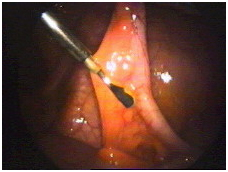
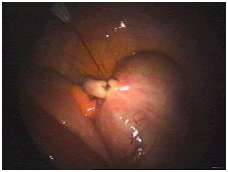
Next, scissors are used to divide the mesentery. Alternating application of the bipolar forceps and scissors allow complete mobilization of the appendix down to its base.
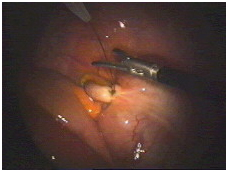
Now the base of the appendix is tied off using a pretied suture which is now being positioned.
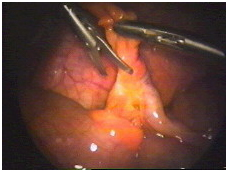
The suture has now been tightened and appears secure. The knot is a fisherman’s knot, which can be tightened, but will not loosen on its own.
As shown in this picture, the suture is now cut with the scissors.
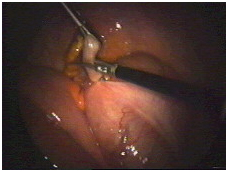
Finally, the appendix is cut free and is ready to be removed.

The operation is complete, and the area is inspected a final time to make sure there is no bleeding.








