The symptoms of exocrine pancreatic cancers and pancreatic neuroendocrine tumors (NETs) are often different, so they are described separately.
Having one or more of the symptoms below does not mean you have pancreatic cancer. In fact, many of these symptoms are more likely to be caused by other conditions. Still, if you have any of these symptoms, it’s important to have them checked by a doctor so that the cause can be found and treated, if needed.
Signs and symptoms of exocrine pancreatic cancer:
Early pancreatic cancers often do not cause any signs or symptoms. By the time they do cause symptoms, they have often already spread outside the pancreas.
Jaundice and related symptoms
Jaundice is yellowing of the eyes and skin. Most people with pancreatic cancer (and virtually all people with ampullary cancer) will have jaundice as one of their first symptoms.
Jaundice is caused by the buildup of bilirubin, a dark yellow-brown substance made in the liver. Normally, the liver excretes bilirubin as part of a liquid called bile. Bile goes through the common bile duct into the intestines, where it helps break down fats. It eventually leaves the body in the stool. When the common bile duct becomes blocked, bile can’t reach the intestines, and the level of bilirubin in the body builds up.
Cancers that start in the head of the pancreas are near the common bile duct. These cancers can press on the duct and cause jaundice while they are still fairly small, which can sometimes lead to these tumors being found at an early stage. But cancers that start in the body or tail of the pancreas don’t press on the duct until they have spread through the pancreas. By this time, the cancer has often spread beyond the pancreas as well.
When pancreatic cancer spreads, it often goes to the liver. This can also lead to jaundice.
Dark urine: Sometimes, the first sign of jaundice is darker urine. As bilirubin levels in the blood increase, the urine becomes brown in color.
Light-colored or greasy stools: Bilirubin normally helps give stools their brown color. If the bile duct is blocked, stools might be pale or gray. Also, if bile and pancreatic enzymes can’t get through to the intestines to help break down fats, the stools can become greasy and might float in the toilet.
Itchy skin: When bilirubin builds up in the skin, it can start to itch as well as turning yellow.
Pancreatic cancer is not the most common cause of jaundice. Other causes, such as gallstones, hepatitis, and other liver and bile duct diseases, are much more common.
Belly or back pain
Pain in the abdomen (belly) or back is common in pancreatic cancer. Cancers that start in the body or tail of the pancreas can grow fairly large and start to press on other nearby organs, causing pain. The cancer may also spread to the nerves surrounding the pancreas, which often causes back pain. Of course, pain in the abdomen or back is fairly common and is most often caused by something other than pancreatic cancer.
Weight loss and poor appetite
Unintended weight loss is very common in people with pancreatic cancer. These people often have little or no appetite.
Nausea and vomiting
If the cancer presses on the far end of the stomach it can partly block it, making it hard for food to get through. This can cause nausea, vomiting, and pain that tend to be worse after eating.
Gallbladder or liver enlargement
If the cancer blocks the bile duct, bile can build up in the gallbladder, making it larger. Sometimes a doctor can feel this (as a large lump under the right ribcage) during a physical exam. It can also be seen on imaging tests.
Pancreatic cancer can also sometimes enlarge the liver, especially if the cancer has spread to the liver. The doctor might be able to feel this below the right ribcage as well on an exam, or it might be seen on imaging tests.
Blood clots
Sometimes, the first clue that someone has pancreatic cancer is a blood clot in a large vein, often in the leg. This is called a deep vein thrombosis or DVT. Symptoms can include pain, swelling, redness, and warmth in the affected leg. Sometimes a piece of the clot can break off and travel to the lungs, which might make it hard to breathe or cause chest pain. A blood clot in the lungs is called a pulmonary embolism or PE.
Still, having a blood clot does not usually mean that you have cancer. Most blood clots are caused by other things.
Fatty tissue abnormalities
Some people with pancreatic cancer develop an uneven texture of the fatty tissue underneath the skin. This is caused by the release of the pancreatic enzymes that digest fat.
Diabetes
Rarely, pancreatic cancers cause diabetes (high blood sugar) because they destroy the insulin-making cells. Symptoms can include feeling thirsty and hungry, and having to urinate often. More often, cancer can lead to small changes in blood sugar levels that don’t cause symptoms of diabetes but can still be detected with blood tests.
Signs and symptoms of pancreatic neuroendocrine tumors:
Pancreatic neuroendocrine tumors (NETs) often release excess hormones into the bloodstream. Different types of tumors make different hormones, which can lead to different symptoms.
Gastrinomas
These tumors make gastrin, a hormone that tells the stomach to make more acid. Too much gastrin causes a condition known as Zollinger-Ellison syndrome, in which the stomach makes too much acid. This leads to stomach ulcers, which can cause pain, nausea, and loss of appetite. Severe ulcers can start bleeding. If the bleeding is mild, it can lead to anemia (too few red blood cells), which can cause symptoms like feeling tired and being short of breath. If the bleeding is more severe, it can make stool black and tarry. Severe bleeding can itself be life-threatening.
If the stomach acid reaches the small intestine, it can damage the cells of the intestinal lining and break down digestive enzymes before they have a chance to digest food. This can cause diarrhea and weight loss.
Glucagonomas
These tumors make glucagon, a hormone that increases glucose (sugar) levels in the blood. Most of the symptoms that can be caused by a glucagonoma are mild and are more often caused by something else.
Excess glucagon can raise blood sugar, sometimes leading to diabetes. This can cause symptoms such as feeling thirsty and hungry, and having to urinate often.
People with these tumors can also have problems with diarrhea, weight loss, and malnutrition. The nutrition problems can lead to symptoms like irritation of the tongue (glossitis) and the corners of the mouth (angular cheilitis).
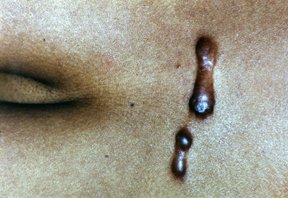
The symptom that brings most people with glucagonomas to their doctor is a rash called necrolytic migratory erythema. This is a red rash with swelling and blisters that often travels from place to place on the skin.
Insulinomas
These tumors make insulin, which lowers blood glucose levels. Too much insulin leads to low blood sugar (hypoglycemia), which can cause symptoms like weakness, confusion, sweating, and rapid heartbeat. When blood sugar gets very low, it can lead to a person passing out or even going into a coma and having seizures.
Somatostatinomas
These tumors make somatostatin, which helps regulate other hormones. Symptoms of this type of tumor can include belly pain, nausea, poor appetite, weight loss, diarrhea, symptoms of diabetes (feeling thirsty and hungry, and having to urinate often), and jaundice (yellowing of the skin and eyes).
The early symptoms of a somatostatinoma tend to be mild and are more often caused by other things, so these tumors tend to be diagnosed at an advanced stage. Often, they are not found until they spread to the liver, when they cause problems like jaundice and pain.
Which treatments are used for pancreatic cancer?
Depending on the type and stage of the cancer and other factors, treatment options for people with pancreatic cancer can include:
- Surgery
- Ablation or embolization treatments
- Radiation therapy
- Chemotherapy and other drugs
Pain control is also an important part of treatment for many patients.
Sometimes, the best option might include more than one type of treatment. To learn about the most common approaches to treating these cancers, see Treating pancreatic cancer, based on the extent of the cancer.
For pancreatic neuroendocrine tumors (NETs), treatment options might include surgery, ablation or embolization treatments, radiation therapy, or different types of medicines. For more on how these tumors are treated, see Treating pancreatic neuroendocrine tumors, based on the extent of the tumor.
 What is Polycystic Ovary Syndrome?
What is Polycystic Ovary Syndrome?