What is a laparoscopic sleeve gastrectomy?
It is an operation to convert the stomach into a long thin tube. This is done by stapling it along its length and then removing the excess. It is performed for helping very overweight patients achieve substantial weight loss because it restricts the amount that someone can eat.
It may be used as a stand-alone operation or the first part of a two stage operation for very large patients. The second stage is carried out a number of months later when the patient has lost a significant amount of weight. This means that the risks of needing further surgical procedures are much less.
What does laparoscopic mean?
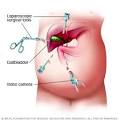
The operation is carried out laparoscopically, which is also known as keyhole surgery. This means that the surgeon makes five small incisions (cuts) in the abdomen (belly) to get to the stomach. The surgeon may decide to convert to an open procedure (the traditional way of carrying out this operation through a longer incision) if they think it would be safer.
What does the operation involve?
The operation takes up to two hours. For some patients, the surgery can be technically difficult depending on body-build or previous surgery. In these circumstances the operation can take longer.
Laparoscopic Sleeve Gasterectomy Surgery in India Cost Hospital
How Is Sleeve Gastrectomy Performed?
We perform the Sleeve Gastrectomy as a laparoscopic procedure. This involves making five or six small incisions in the abdomen and performing the procedure using a video camera (laparoscope) and long instruments that are placed through these small incisions.
During the Laparoscopic Sleeve Gastrectomy, about 75% of the stomach is removed leaving a narrow gastric “tube” or “sleeve”. No intestines are removed or bypassed during the sleeve gastrectomy.The LSG takes one to two hours to complete.
How Does Sleeve Gastrectomy Cause Weight Loss?
Sleeve Gastrectomy is a restrictive procedure. It greatly reduces the size of your stomach and limits the amount of food that can be eaten at one time. It does not cause decreased absorption of nutrients or bypass your intestines. After eating a small amount of food, you will feel full very quickly and continue to feel full for several hours.
Sleeve Gastrectomy may also cause a decrease in appetite. In addition to reducing the size of the stomach, Sleeve Gastrectomy may reduce the amount of “hunger hormone” produced by the stomach which may contribute to weight loss after this procedure.
Laparoscopic Sleeve Gasterectomy Surgery in India Cost Hospital
Who Do We Offer Laparoscopic Sleeve Gastrectomy?
This procedure is primarily used as part of a staged approach to surgical weight loss. Patients who have a very high body mass index (BMI) or who are at risk for undergoing anesthesia or a longer procedure due to heart or lung problems may benefit from this staged approach. Sometimes the decision to proceed with a two-stage approach is made before surgery due to these known risk factors. In other patients, the decision to perform sleeve gastrectomy (instead of gastric bypass) is made during the operation. Reasons for making this decision intraoperatively include an excessively large liver or extensive scar tissue that would make the gastric bypass procedure too long or unsafe.
In patients who undergo LSG as a first stage procedure, the second stage (gastric bypass) is performed 12 to 18 months later after significant weight loss has occurred and the risk of anesthesia is much lower (and the liver has decreased in size). Though this approach involves two procedures, we believe it is safe and effective for selected patients.
Laparoscopic Sleeve Gastrectomy can also be used as a primary procedure. There is relatively little data regarding the use of LSG as a stand-alone procedure in patients with lower BMI’s and it should be considered an investigational procedure in this patient group. We are offering this procedure to diabetic patients with a BMI between 30 and 40 as a part of a clinical trial that will better define the short and long-term benefits of LSG in this group of patients.
What Are The Risks Of Laparoscopic Sleeve Gastrectomy?
There are risks that are common to any laparoscopic procedure such as bleeding, infection, injury to other organs, or the need to convert to an open procedure. There is also a small risk of a leak from the staple line used to divide the stomach. These problems are rare and major complications occur less than 1% of the time.
Overall, the operative risks associated with LSG are slightly higher than those seen with the laparoscopic adjustable band but lower than the risks associated with gastric bypass.
What Are The benefits Of Laparoscopic Sleeve Gastrectomy?
Depending on their pre-operative weight, patients can expect to lose between 40% to 70% of their excess body weight in the first year after surgery.
Many obesity-related comorbidities improve or resolve after bariatric surgery. Diabetes, hypertension, obstructive sleep apnea and abnormal cholesterol levels are improved or cured in more than 75% of patients undergoing LSG. Though long-term studies are not yet available, the weight loss that occurs after LSG results in dramatic improvement in these medical conditions in the first year after surgery.
Is Laparoscopic Sleeve Gastrectomy A Good Choice For Me?
Your surgeon may talk to you about LSG as an option if you have a BMI over 60 or significant medical problems that increase your risk for undergoing anesthesia or gastric bypass. Laparoscopic Sleeve Gastrectomy may also be offered as part of a clinical investigation if you have a lower BMI and diabetes.