Overview
You may know pressure sores by their more common name i.e, bedsores, pressure ulcers and decubitus (‘lying down’) ulcers. Bedsores can arise over hours or days. Pressure sores are areas of damage to the skin and the underlying tissue caused by constant pressure or friction. This type of skin damage can develop quickly to anyone with reduced mobility, such as older people or those confined to a bed or chair.
It affects the skin over bony areas such as the heels, elbows, the back of the head and the tailbone (coccyx) is particularly at risk. The lack of enough blood flow can cause the affected tissue to die if left untreated. Pressure sores can be difficult to treat and can lead to serious complications. Pressure sores are graded to four levels, If found early, there’s a good chance these sores will heal in a few days, with little fuss or pain. Without treatment, they can get worse. Most sores heal with treatment, but some never heal completely. You can take steps to put a stop to bedsores and help them heal.
Warning signs of pressure sores
Daily checks are needed to look for early warning signs including:
- red, purple or blue torn or swollen skin, especially over bony areas
- signs of infection, such as skin warmth, swelling, cracks, calluses, and wrinkles.
Pressure Sores Diagnosis
- When did the sore appear?
- Does it hurt?
- How often do you change positions?
- Have you ever had a pressure sore before?
Pressure Sores Stages/Grades and their Symptoms
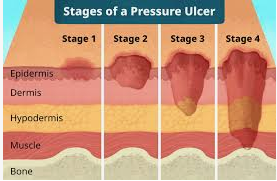
There are four stages of pressure sores from mild to severe:
Stage I
This is the mildest stage. These pressure sores only affect the upper layer of your skin.
Symptoms: Pain, burning, or itching are common symptoms. The spot may also feel different from the surrounding skin: firmer or softer, warmer or cooler.
You may notice a red area on your skin. If you have darker skin, the discolored area may be harder to see. The spot doesn’t get lighter when you press on it or even 10-30 minutes after you stop pressing. This means less blood is getting to the area.
Stage II
This happens when the sore digs deeper below the surface of your skin.
Symptoms: Your skin is broken, has an open wound, or looks like a pus-filled blister. The skin around it may be discolored.
The area is swollen, warm, and/or red. The sore may ooze clear fluid or pus. And it’s painful.
Stage III
These sores have gone through the second layer of skin into the fat tissue.
Symptoms: The sore looks like a crater and may have a bad odor. It may show signs of infection: red edges, pus, odor, heat, and/or drainage. The tissue in or around the sore is black if it has died.
Stage IV
These sores are the most serious. Some may even go so deep they affect your muscles, ligaments, and bones.
Symptoms: The sore is deep and big. Skin has turned black and shows signs of infection—red edges, pus, odor, heat, and/or drainage. You may be able to see tendons, muscles, and bone.
Other stages
In addition to the four main stages for bed sores, there are two others:
Unstageable is when you can’t see the bottom of the sore because it’s covered in a layer of dead skin. Your doctor can only stage it once it’s cleaned out.
Suspected deep tissue injury is when the surface of the skin looks like a stage I or II sore, but underneath the surface, it’s a stage III or IV sore.
Risk factors for pressure sores
A pressure sore is caused by constant pressure applied to the skin over a period of time. The skin of older people tends to be thinner and more delicate, which means an older person has an increased risk of developing a pressure sore during a prolonged stay in bed.
Other risk factors for pressure sores include:
- immobility and paralysis – for example due to a stroke or a severe head injury
- being restricted to either sitting or lying down
- impaired sensation or impaired ability to respond to pain or discomfort. For example, people with diabetes who experience nerve damage are at increased risk of pressure sores
- urinary and faecal incontinence – skin exposed to urine or faeces is more susceptible to irritation and damage
- malnutrition – can lead to skin thinning and poor blood supply, meaning that skin is more fragile
- obesity – being overweight in combination with, for example, immobility or being restricted to sitting or lying down can place extra pressure on capillaries. This then reduces blood flow to the skin
- circulation disorders – leading to reduced blood flow to the skin in some areas
- smoking – reduces blood flow to the skin and, in combination with reduced mobility, can lead to pressure sores. The healing of pressure sores is also a slower process for people who smoke.
If you use a wheelchair you’re most likely to develop a pressure sore on the parts of the body where they rest against the chair. These may include the tailbone or buttocks, shoulder blades, spine and the backs of arms or legs.
If you’re bedridden, pressure sores can occur in a number of areas, including:
- back or sides of the head
- rims of the ears
- shoulders or shoulder blades
- hipbones
- lower back or tailbone
- backs or sides of the knees
- heels, ankles and toes.
Treatment for pressure sores
There are a variety of treatments available to manage pressure sores and promote healing, depending on the severity of the pressure sore. These include:
- regular position changes
- special mattresses and beds that reduce pressure
- being aware of the importance of maintaining healthy diet and nutrition
- dressings to keep the sore moist and the surrounding skin dry. There is no advantage of one type of dressing over another.
- saline gauze dressing may be used if ointments or other dressings (for example foam dressings) are unavailable.
- light packing of any empty skin spaces with dressings to help prevent infection
- regular cleaning with appropriate solutions, depending on the stage of the sore
- there is no advantage of one particular type of antiseptic (e.g. iodine) or antibiotic treatment over another
- specific drugs and chemicals applied to the area, if an infection persists
- surgery to remove the damaged tissue that involves thorough debridement of the wound, the removal of underlying or exposed bone, and filling the empty space
- operations to close the wound, using skin grafts if necessary
- continuing supportive lifestyle habits such as eating a healthy and nutritious diet, as suggested by the nutritional staff.
Preventing pressure sores
If you are confined to a bed or chair for any period of time, it’s important to be aware of the risk of pressure sores. To prevent skin damage, you or your carer need to relieve the pressure, reduce the time that pressure is applied and improve skin quality. Pressure offloading surfaces such as mattresses and wheelchair cushions may help in providing pressure relief by evenly distributing the pressure.
Pressure injury monitoring devices that measure the skin moisture content, body motion and the pressure in-between may be used to prevent pressure sores and injuries. An example of a devices is pressure-sensing mats placed on beds or wheelchairs.
Develop a plan that your, your carer and any other caregivers can follow. This plan will include position changes, supportive devices, daily skin care, a nutritious diet and lifestyle changes.
A routine nursing assessment may be required if you’re at high risk of pressure sores. As visual skin assessment may sometimes be unreliable, early detection of pressure sores using some bedside technologies may help facilitate preventive interventions.
Pressure from medical devices such as oxygen tubing, catheters, cervical collars, casts and restraints should be minimised or removed.
Position changes to prevent pressure sores
If you use a wheelchair shift position within your chair about every 15 minutes. If you spend most of their time in bed change position at least once every two hours, even during the night and avoid lying directly on your hipbones.
Pillows may be used as soft buffers between your skin and the bed or chair. The head-of-bed elevation should be maintained at/or below 30 degrees. Or depending on the your medical condition, the bed should at least be elevated to the lowest degree to prevent injury. When lying on your side, a 30 degrees position should be used.
Daily skin care to prevent pressure sores
Ways to prevent pressure injuries include:
- Checking the skin at least daily for redness or signs of discolouration.
- Keeping the skin at the right moisture level, as damage is more likely to occur if skin is either too dry or too moist.
- Using moisturising products to keep skin supple and prevent dryness.
- Never massaging bony areas because the skin is too delicate.
Diet and lifestyle changes to avoid pressure sores
Changes to avoid pressure sores include:
- Make sure you eat a healthy and nutritious diet. This includes a balanced diet (proteins, fats and carbohydrates) and fluids/water. And if necessary,you’re your doctor about vitamin and nutritional supplements (e.g. zinc, antioxidants).
- Low body weight or being overweight can cause pressure sores, so make sure you maintain heathy body weight
- If you’re malnourished or at risk of malnutrition, protein, fluid and energy intake should be increased.
- Be aware of using good hygiene practices.
- Maintain activity levels, where appropriate.
- Make sure you quit smoking.
Tips for skin care
Consider these suggestions for skin care:
- Keep skin clean and dry. Wash the skin with a gentle cleanser and pat dry. Do this cleansing routine regularly to limit the skin’s exposure to moisture, urine and stool.
- Protect the skin. Use moisture barrier creams to protect the skin from urine and stool. Change bedding and clothing frequently if needed. Watch for buttons on the clothing and wrinkles in the bedding that can irritate your skin.
- Inspect the skin daily. Look closely at your skin daily for warning signs of a bedsore.
Further for any queries in regards to the medical assistance please feel free to email us on query@gtsmeditour.com or you can whatsapp us on +91 9880149003.
Thank you..!