Cancer happens when there is uncontrolled growth of abnormal cells that thrive and spread instead of dying as they would in the life cycle of a normal cell.
Lymphoma is a cancer that starts in the white blood cells, or lymphocytes.
Lymphatic cancers are classified by the type of immune cells affected. The two main types are Hodgkin and non-Hodgkin. Within these, there are many subtypes.
Non-Hodgkin, the most common type, affects B and T cells. Classic Hodgkin lymphoma is marked by the presence of cells known as Reed-Sternberg cells. Other subtypes affect different types of cells.
Hodgkin can occur at any age, but it is most common in children and adults under 25 years. It affects men more than women. In most cases, it is curable, but treatment and prognosis vary between sub types.

Tumor Stages are below:
Symptoms
The signs and symptoms of lymphoma are similar to those of illnesses such as viral diseases and the common cold, but they continue for longer than would normally be expected.
Some people will have no symptoms, but some may notice a swelling of the lymph nodes. These are located all around the body, often in the neck, groin, abdomen, or armpits.
The swellings are normally painless, but pain may occur if the enlarged glands press on organs, bones, and other structures. This can be confused with back pain.
Lymph nodes can swell during common infections, such as a cold, but in lymphoma the swelling does not go away. Pain is also more likely to accompany the swelling if it is due to an infection.
The overlap of symptoms can lead to misdiagnosis.
Anyone who has ongoing swelling of the glands should see their doctor.
Other symptoms of both types of lymphoma may include:
- ongoing fever without infection
- night sweats, fever, and chills
- weight loss and loss of appetite
- unusual itching
- persistent fatigue, unusual tiredness, or lack of energy
- pain in lymph nodes after drinking alcohol
Additional symptoms that can indicate Non-Hodgkin lymphoma include:
- persistent coughing
- shortness of breath
- pain or swelling of the abdomen
Pain, weakness, paralysis, or otherwise altered sensation can occur if an enlarged lymph node presses against spinal nerves or the spinal cord.
Lymphoma can spread rapidly from the lymph nodes to other parts of the body through the lymphatic system. As cancerous lymphocytes spread into other tissues, the body’s ability to fight infection weakens.
Causes and risk factors
Exactly what causes lymphoma is unclear, but there are some risk factors.
Non-Hodgkin lymphoma
Risk factors for non-Hodgkin lymphoma include:
- Age: Most lymphomas occur in people aged 60 years and older, but some types are more likely to affect children and young adults.
- Sex: Some types are more likely in women, others are more likely in men.
- Ethnicity and location: It is more common in developed nations.
- Chemicals and radiation: Nuclear radiation and some chemicals used in agriculture have been linked to non-Hodgkin lymphoma.
- Immunodeficiency: A person with a weak immune system is more at risk. This can be due, for example, to HIV ro AIDS, medications taken after an organ transplant.
- Autoimmune disease: This is when the immune system attack the body’s own cells. Examples include rheumatoid arthritis and celiac disease.
- Infection: Certain viral and bacterial infections that transform lymphocytes increase the risk, such as the Epstein-Barr virus (EBV), which causes glandular fever.
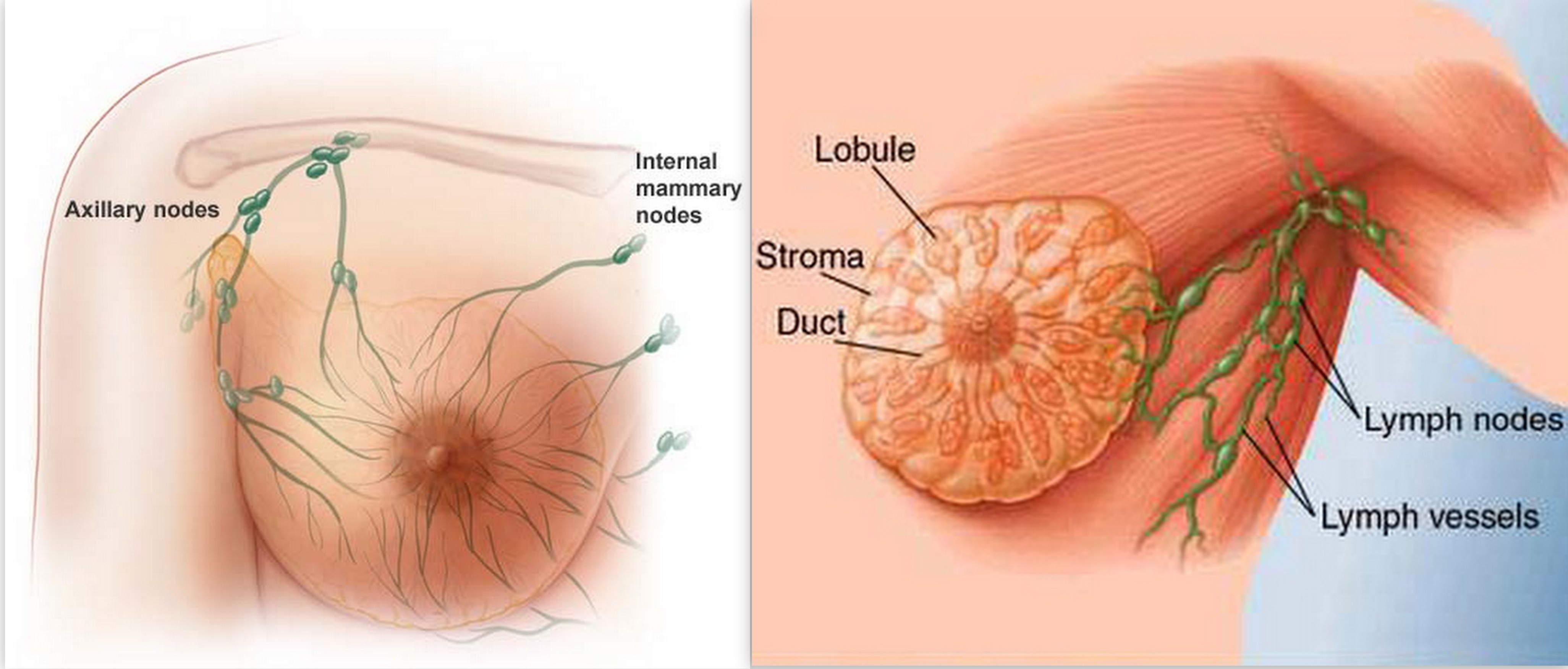
- Breast implants: These can cause anaplastic large cell lymphoma in the breast tissue.
- Body weight and diet: Obesity has been implicated in the development of lymphoma, although more research is needed to confirm the link.
Hodgkin lymphoma
Risk factors for Hodgkin lymphoma include:
- Infectious mononucleosis: Infection with EBV can cause mononucleosis, which increases the risk of lymphoma.
- Age: People between the ages of 20 and 30 years and people over the age of 55 years have a higher risk
- Sex: It is slightly more common in men.
- Location: Hodgkin lymphoma is most common in the U.S., Canada, and northern Europe. It is least common in Asia.
- Family: If a sibling has the condition, the risk is slightly higher, and very high if the sibling is an identical twin.
- Affluence: People from higher socioeconomic status are at greater risk
- HIV infection: This can weaken the immune system and increase the risk of lymphoma.
Spread of lymphoma
Lymphatic tissue is connected throughout the body, and the cancer cells can spread easily from their original location to other tissues and organs, including those outside of the lymphatic system.
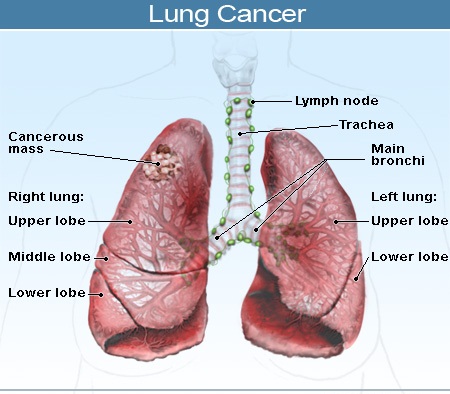
Lymphoma most often spreads to the liver, bone marrow, or lungs.
In Hodgkin lymphoma, this spread usually affects one lymph node after another in order.
In non-Hodgkin lymphoma, tumors may arise in disparate lymph nodes, skipping some nodes.
Tests for lymphoma
Tests will confirm whether lymphoma is present.
Blood tests and biopsies can detect the presence of lymphoma and distinguish between them.
A biopsy involves taking a sample of lymph tissue for examination in a laboratory. The surgeon may remove a whole lymph or a part of one. In some cases, a needle can be used to take a tissue sample. A bone marrow biopsy may be necessary. This may need a local anesthetic, a sedative, or a general anesthetic.
Biopsies and other tests can confirm the stage of the cancer, to see whether it has spread to other parts of the body.
Imaging tests such as a CT or MRI scan, X-ray imaging of the chest, abdomen, and pelvis, ultrasound scanning, or a PET scan.
A spinal tap, where a long, thin needle is used under local anesthetic to remove and test spinal fluid.
Staging of the cancer depends on the type, growth rate, and cellular characteristics. In stage 0 or I, the cancer is confined to a small area. In stage 4, it has spread to more distant organs.
Lymphoma can also be described as indolent, limited to one place, or aggressive, spreading to other parts of the body.
Treatment:
Treatment depends on the type of lymphoma and the stage it has reached. Indolent, or slow-growing lymphoma may need only watchful waiting and no treatment.
If treatment is necessary, it can involve:
- Biologic therapy: This is a drug treatment that stimulates the immune system to attack the cancer cells by inserting living microorganisms into the body.
- Antibody therapy: Synthetic antibodies are inserted into the bloodstream to combat the cancer’s antigens.
- Chemotherapy: Aggressive drug treatment is used to kills cancer cells.
- Radioimmunotherapy: This delivers high-powered radioactive doses directly into the cancerous B-cells and T-cells to destroy them.
- Radiation therapy: This is used to focus on small areas of cancer.
- Stem-cell transplantation: This can restore damaged bone marrow following high-dose chemotherapy or radiation therapy.
- Steroids: These may be injected to treat lymphoma.
- Surgery: This can be used to remove the spleen or other organs after the lymphoma has spread.
Surgery is used more often for obtaining a biopsy.



.jpg)